
The Machine That Stops His Heart to Save It
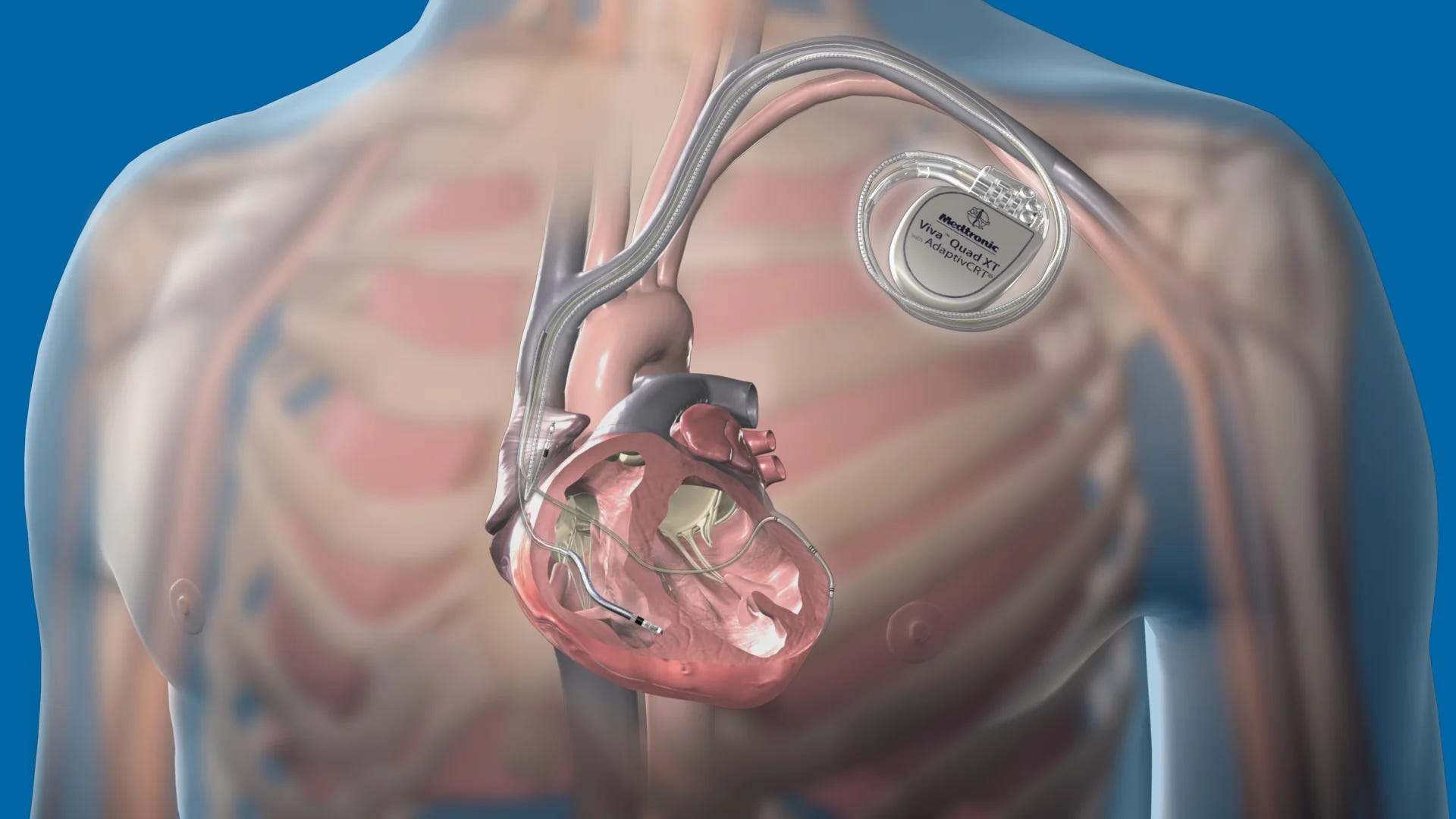
His own heart was trying to kill him. The answer was a matchbox under his collarbone, a three-volt cell, and a trick borrowed from Faraday.

I had just finished my floor and come down to the cardiac unit. I had been there maybe a minute when the monitor over one of the beds started to alarm.
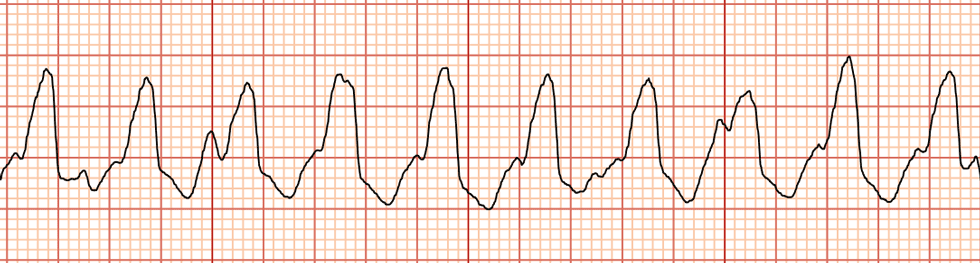
The line on the screen had lost its shape. Where there should have been the clean, spaced beat of a normal rhythm, there was a fast, wide, frantic scribble. Ventricular tachycardia. A heart beating so fast it can no longer fill, no longer pump, no longer keep you alive. Left alone, it kills in minutes.
The room moved the way rooms move when everyone is afraid and pretending not to be. I asked the nurse one question. Does he have an ICD. She said yes.
So we waited.
That was the part I was not ready for. You stand over a man whose own heart is trying to kill him, and you do nothing. You wait, because the small titanium box buried under his collarbone has already seen it, faster than any of us, and it has already started doing something. We just could not see it yet.
Then he screamed.
And it worked. We looked at the monitor and the frantic scribble was gone, replaced by the slow, ordinary, almost beautiful line of a heart that had remembered itself.
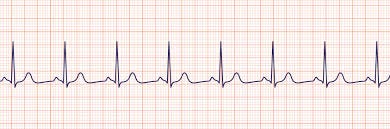
This is the most comforting image in cardiology.
The room exhaled. The thing that made him scream was the same thing that saved him. They were not two events. They were one.
I wish that had been the end of it. A few minutes later the monitor alarmed again. The box did its work again. He screamed again. Normal again. A medication that controls the heart electrophysiology was started. And yet, It happened five times.
By the third, the relief had drained out of the room and left only the dread, because now we knew. We knew the alarm was coming. We knew the silence before it was coming. We knew he would scream. And there was nothing for any of us to do but stand there and trust a piece of metal to hurt him back to life one more time.
This has a name. When a heart throws three or more of these in a single day, we call it an electrical storm. He weathered five before the medications finally pulled him out of it. Now, he went home. He is stable. And he will carry that box for the rest of his life.
The physics part of the implanted ICD is actually one of the most interesting parts you’ll learn and it’s what we’re covering today.
To drag a fibrillating heart back into rhythm, you have to push something like 35 joules through it in about ten milliseconds. ONLY 10 milliseconds.
Run that. Power is energy divided by time, so it works out to 35 joules spent in a hundredth of a second. Three and a half thousand watts. A peak of roughly fifteen amps, briefly drawing more power than everything in your kitchen at once, routed straight through a human chest. So how come all this energy is stored in this small box? It’s not, and that’s the brilliant part in its creation.
The secret is a key distinction of energy versus power.
Energy is how much you have. Power is how fast you can deliver it. Those are two completely separate things, and the whole device is built on the gap between them.
Picture a tap dripping into a bucket. The drip is pathetic. You could never put out a fire by pointing that tap at the flames. But let it run long enough and the bucket fills, and a full bucket thrown all at once is nothing like a drip.
The ICD’s battery is that tap. At any single moment it can only push out a thin trickle of current, and that is exactly why it can survive inside the body for nearly ten years. Add that trickle up across all those years and the total energy is enormous. But ask for all of it in one instant, the thousands of watts a shock needs, and the battery simply cannot do it. Its chemistry is too slow. It has the energy. It does not have the power. I’m not saying it charges for years before each shock. NO as I said the patient got shocked 5 times in a day and it was even just planted earlier in the morning. But it has the capacity for this energy.
The device never shocks you straight from the battery. It spends a few seconds quietly letting that weak trickle fill a bucket, and then it throws the whole bucket in a single instant.
That bucket is the capacitor and it does the storing. How much energy it can hold follows one of the cleanest equations in physics: E = ½CV². Notice that the energy climbs with the square of the voltage, which means voltage is where all the leverage hides. Take a real ICD capacitor, around 125 microfarads (unites of capacitance), and ask what voltage you need to bank 35 joules in it. Rearrange to V = √(2E/C) and the answer comes out near 750 volts.
Seven hundred and fifty volts. Built inside a box that runs on three.
So the ICD finds out the heart is out of rhythm and with it’s 3 volt, it charges a capacitance of 750? How? Voltage does not stack like coins. But we can do something smart here.
Let the 3 volts drive current through a tiny coil, then switch it off sharply, over and over, tens of thousands of times a second. The useful fact is this: every time the current through that coil changes, it induces a voltage in a second coil wound right beside it. That is Faraday’s law, EMF = −N·dΦ/dt, the single idea most of modern civilization quietly runs on. Give that second coil far more loops than the first, the big N in the equation, and the voltage comes out multiplied.
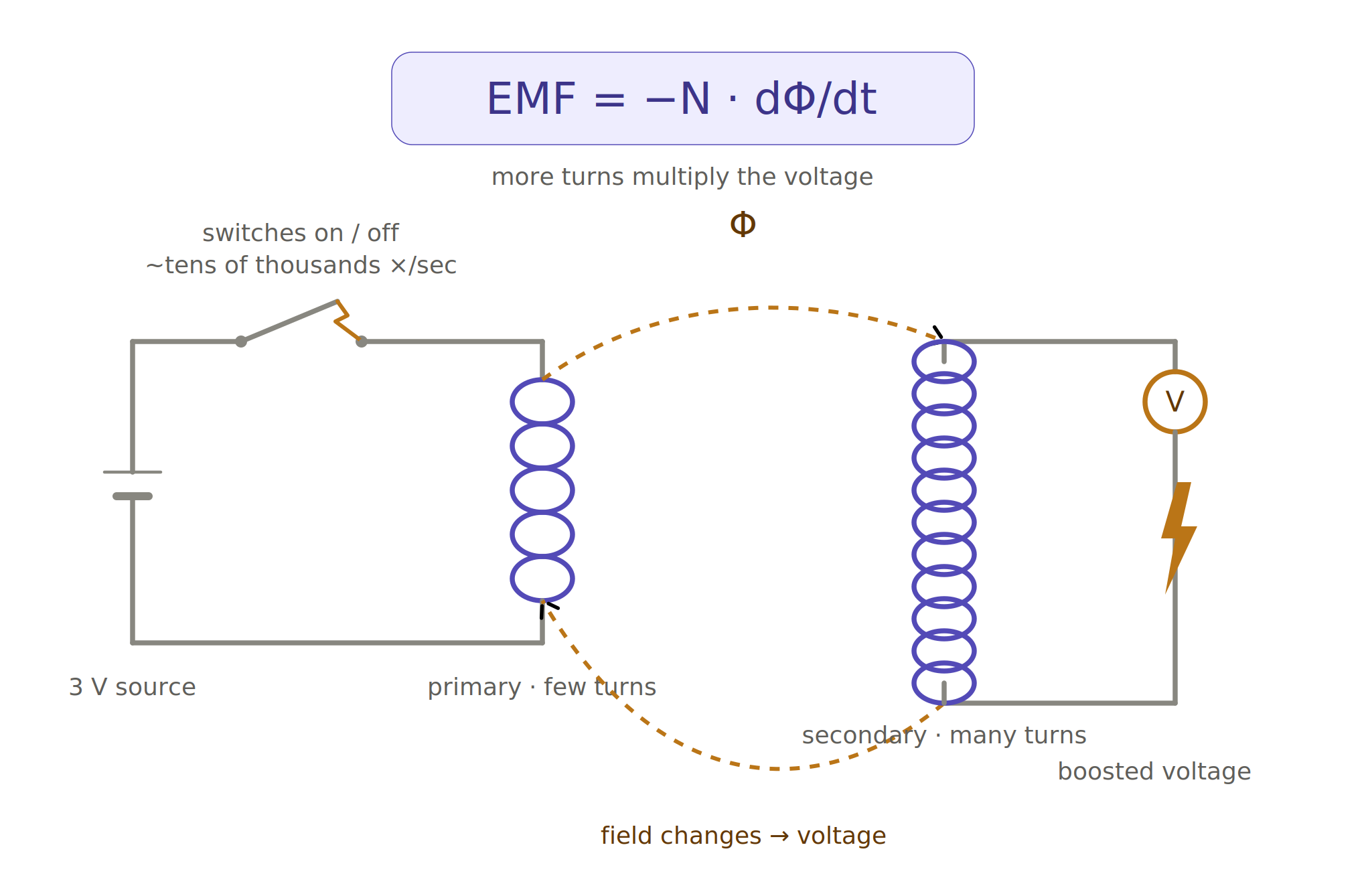
Each on-off cycle stores a little energy in the coil’s magnetic field, E = ½LI², and pushes a pulse of it into the capacitor. The voltage climbs. Three becomes a hundred becomes five hundred becomes seven fifty, one magnetic pulse at a time.
And it takes a few seconds.
That is the silence from earlier. The pause we stood inside, doing nothing, waiting. The box was not hesitating. It was inducting. Climbing to 750 volts by the only road physics allows, and there is no faster one. The wait was not a flaw. It was the law.
Then it lets go.
The heart and the wires touching it behave, electrically, like a plain resistor, somewhere near 50 ohms. So the capacitor does not empty in an instant. It drains the way every capacitor drains, exponentially: V(t) = V₀·e^(−t/RC). Built into that is a natural clock, the time constant τ = RC, which for these numbers is about six milliseconds. That is the shock. Not a spark, not a held current. A six-millisecond exponential collapse of stored voltage across a living heart.
But none of that answers the real question. Why does a jolt of electricity fix a heart at all? Electrocuting an organ that is already failing electrically sounds like the last thing you would ever want to do.
The answer is the most beautiful idea in this whole story, and it has almost nothing to do with the box.
Your heart is what physicists call an excitable medium. A normal beat is a single, organized wave of activation sweeping across the muscle from one corner, each cell handing the signal to the next and then going briefly numb, so the wave only ever moves forward. One clean wave, one squeeze.
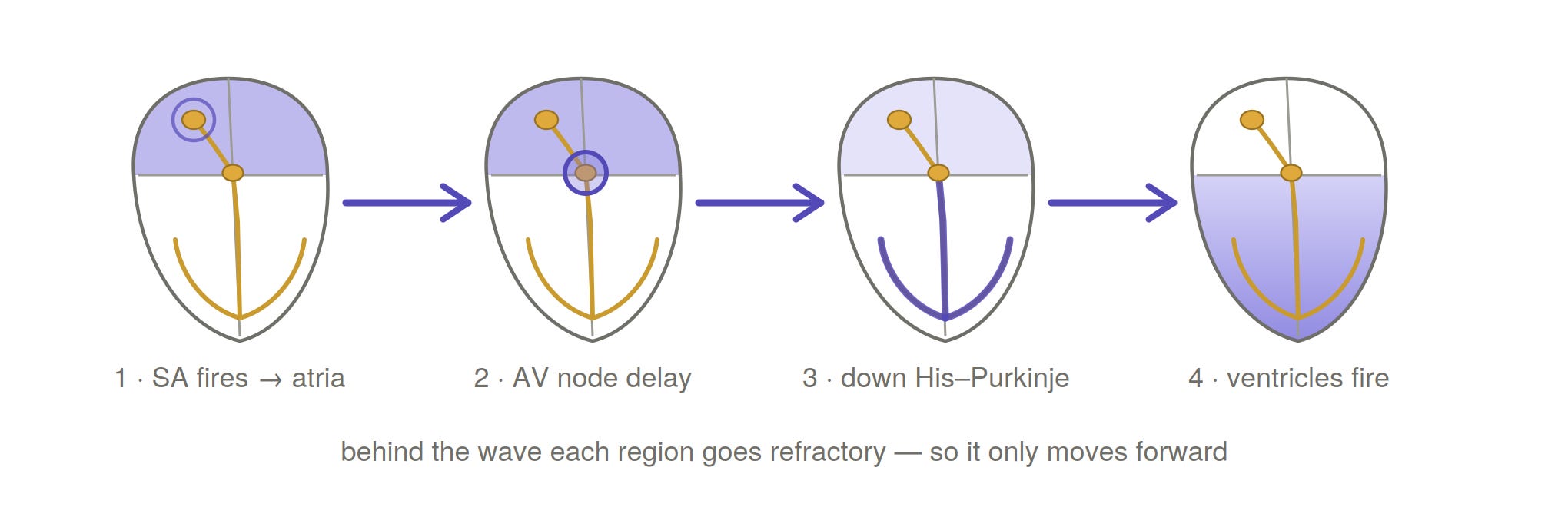
In ventricular tachycardia, that wave stops moving in a line and starts chasing its own tail, looping the same circuit over and over. In fibrillation it shatters outright into spinning spiral waves, called rotors, each one whipping around and re-firing the tissue the instant it recovers. The heart is not stopped. It is too busy. Every patch of it contracts at a different moment, so nothing actually pumps. It quivers. The exact same spiral-wave mathematics turns up in certain chemical reactions, the famous Belousov-Zhabotinsky reaction swirling in a dish, which means the thing trying to kill this young man is, underneath, a pattern, not a poison.
You cannot reason with a rotor. You cannot ask it to stop. So you do the one thing that works. You depolarize almost the entire heart at once. The shock slams the overwhelming majority of the muscle into that brief numb state simultaneously, all of it, in a single instant. And a spinning wave with nowhere left to spin simply dies. The chaos runs out of tissue to feed on. The heart falls silent for a fraction of a second, and then the natural pacemaker, finally unobstructed, lays down a clean wave again.
So the shock does not restart the heart. It does the opposite. It stops everything, all at once, so that order has room to come back on its own.
Even the length of the shock is not arbitrary. The membrane wrapped around every heart cell is itself a tiny capacitor, and it takes a few milliseconds to charge. So the pulse is tuned to that. Long enough to actually move the membranes, short enough not to waste energy. Six milliseconds is not a number an engineer chose. It is a number the cell chose, and the engineer listened.
There is, for what it is worth, a gentler version of all this. When the problem is a single looping circuit, the box can sometimes end it with no shock at all. It paces the heart faster than the arrhythmia, sending in its own waves timed to crash head-on into the runaway one and cancel it out. A wave used to kill a wave, in silence, often without the patient feeling anything. Our patient did not get that mercy. His heart needed the full 750 volts, five times over. But it is worth knowing the box tries to be kind when it can.
And every bit of this rests on the box being right in the first place. Before it charges anything, it has to read the heart’s electrical whisper, a signal measured in thousandths of a volt, count the spacing of the beats, weigh their shape, and decide in a moment whether this is a lethal rhythm, or a frightened heart simply beating fast, or nothing but electrical noise. It must never miss the real thing and never fire on a healthy one. It makes that call faster than anyone standing at the bedside could.
So put it together. Under that young man’s collarbone sits a machine that runs on induction, hoards energy in a magnetic field, banks it in an electric one at 750 volts, spends it on a six-millisecond clock set by the laws of capacitance, and uses it to silence a chaotic wave pattern by forcing an entire organ into a single instant of agreement. All of it the size of a matchbox. All of it deciding, for years, faster than a human ever could.
We understand every step of that chain. We can write the equation for each one. And we still cannot tell that young man why his heart was built to do this, or when it will reach for it again. We have engineered something close to a miracle for the rescue. We remain mostly in the dark about the thing it rescues him from.
On Thursday, I want to go after exactly that, the thing the box rescues him from.
We’ll turn the camera off the machine and onto the heart itself, starting from the very beginning. What a single heartbeat actually is as a wave of electricity, why the ECG traces the precise shape it does, and what every bump and spike on that monitor is really telling you. Then we’ll watch that clean wave come apart, one physical step at a time, until we are standing back at the exact moment from today, the frantic scribble of ventricular tachycardia, only this time you will understand precisely how a healthy heart talks itself into trying to die.
The beginning is free. The full walk, from the first wave all the way to the final shock, is for paid subscribers.
Beautifully written and although I don’t pay you anything: I liked the medicine/physics mix. I had an transvenous icd for years, never did anything, then got infected with streptococcus aureus. It had to go and now rests on my desk. Tomorrow I will get the subcutane variant without the possibility for pacing.
I still hope it is just insurance on the long run. 3kW don’t seem nice at all.
retired utility engineer here. LOVE your stuff. I’m a paid subscriber. I believe power is instantaneous and energy is power TIMES time. 1 MW constant over an hour is 1 MWh. Otherwise excellent article!